We research and develop technical solutions to monitor and remove gas bubbles in viscous fluids.
Our flagship concept Emboless® passively separates fluids of different density. Developed to reduce air infusions in blood lines, but can be used in a wider spectrum of applications. Such example could be separating air or water from an oil flow.
The Emboless® concept
A degassing chamber for significant reductin of microbubbles in any fluid such as blood, infusion fluids, drug development and technical procedures.
Applicable for clinical use such as for acute and chronic haemodialysis, apheresis procedures, infusion technology and technical equipment.
Microbubble complications
Air contamination of the blood of the patient appears in conjunction with infusion of fluid, injections of drugs and during extracorporeal treatments such as dialysis, apheresis, and cardio-pulmonary bypass.
Larger amounts may lead to instant death while smaller amounts such as microbubbles will cause microemboli by the gas bubble itself and further by the attached clot that appears around and attached to the bubble (See figure).
A single microemboli will cause a local damage in the tissue where it deposits. If this is the lung, a scar will develop but experienced side effects may recover with no or limited side effects to the patient. If the localization of the microemboli is in a crucial part of the body such as regulating center in the heart or brain severe consequences may appear, such as sudden death or a crucial stroke.
Numerous microbubble exposures could lead to tissue damage that will sum up over time, causing progressive organ damage.
To limit gas exposure the concept of including a venous chamber in a blood line before the blood or infusion fluid returns to the patient was introduced to enable air/gas to evaporate out of the fluid already in the 1950th…?
However, we have investigated venous chambers in clinical use for dialysis and found that the efficacy to remove air bubbles is strongly limited (See laboratory work, Jonsson et al 2023). Most dialysis devices do not alarm for microbubble contamination if the size of a bubble is less than 500µm diameter.
Bubble reduction
In a Fresenius 5008 venous chamber the blood flow enters from the top and exits at the bottom. Microbubbles then push against their lift force downwards by the blood flow.
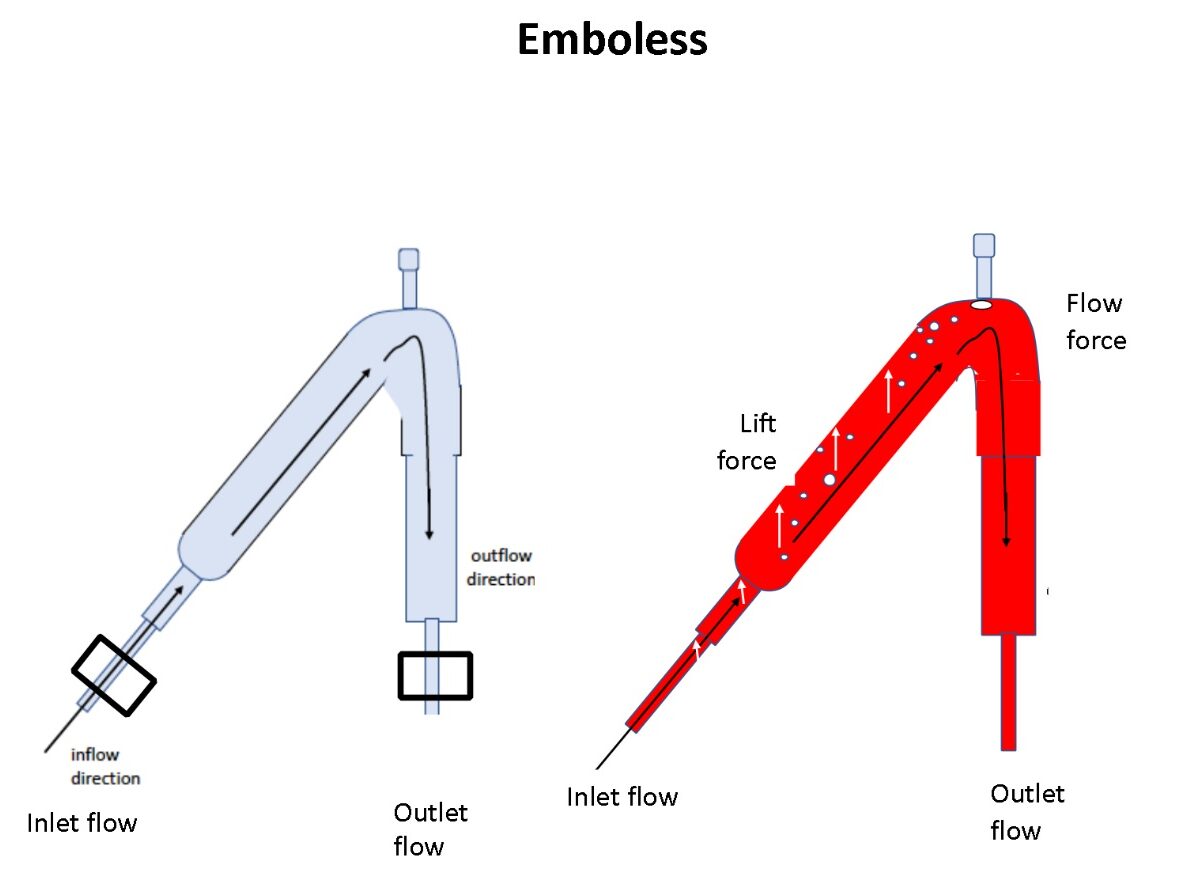
In the Emboless® venous chamber the blood flow enters from above towards the top before turning downwards to the exit. In the rising blood flow part of the chamber, the lift force of gas bubbles are supported to merge and retain at the top.
Laboratory experiments
The contamination of air within the closed extracorporeal dialysis system was described Jonsson in his Thesis. During – recirculation of dialysis priming fluid ? in … minutes 6 ml of air was consolidated and isolated from the circuit.
A viscous fluid was prepared by saline, sepharos …. and albumin ..%, to be used at room temperature but to mimic the viscosity of the blood (referens). This fluid was able to show that ultrasound detection of microemboli were due to microbubbles (the fluid is devoid of blood and therefore counts couldn’t be made by blood clots).
It was now possible to visualize larger microbubbles passing the air trap without inducing an alarm and entering the sieve of the venous chamber. (see movie).
Follow up experiments visualized that the shape of air traps and the pump speed of the fluid in the extracorporeal circuit influenced the contamination of microbubbles of air at the Inlet and Outlet side (C Stegmayr et al 2007).
Further a primed but originally dry dialyzer caused a greater amount of inlet microbubbles than a wet stored gamma sterilized dialyzer (C Stegmayr et al 2008).
Priming of more than 3 L was necessary to achieve a considerable reduction of bubbles in the extracorporeal circuit (C Stegmayr et al )
These results showed that air contamination appeared into the blood by a whipping cream effect caused by the fluid entering the vanous chamber from the top (see figure)
Various experimental studies were performed to define differences in shape to optimize reduction of microbubbles by a specific chamber for the venous blood return. This resulted in a designs that was patented and named Emboless® (oklart hur mycket vi refererar till).
A follow up in vitro study was performed to compare four frequently used extracorporeal circuits, with different shapes of venous chambers, with the Emboless® chamber. Compared devices and their extracorporeal tubing systems were Baxter Artis, Baxter AK78, Fresenius 5008 and Fresenius 6008.
The Emboless most efficiently eliminated the microbubbles (Jonsson 2023). Again a higher blood pump speed had significant worse impact on the outcome.
Clinical experiments
Measurement of microbubbles in the return line after the venous chamber verified high amounts of microbubbles that were higher/worse if the blood pump speed used for the specific patient was higher. (Stegmayr 2007)
Since it was generally stated that air bubbles resorbed when entering the body we performed a study microbubble count measuring bubble count by a hand-held probe and ultrasound signals. A significant increase in microembolic signals were found after start of dialysis at the vascular access but also at the external carotic artery (Forsberg 2010)
In a clinical interventional study we showed that using a wet dialyzer caused less microbubble contamination in the blood return line of the patient. In addition the use of a low blood level in the venous chamber of the Fresenius 5008 blood line cause significantly more microbubble counts in the return line (Forsberg 2013).
A follow up and blinded study using a high versus low blood level in the venous chamber showed significant better results for a high blood level (Forsberg 2012).
In an overview study ultrasound measurements were performed to evaluate where microbubble counts were expected to enter the extracorporeal bloodline during dialysis showed addition of signals at the vascular access site, within the bloodline where a negative pressure existed, after the dialyzator, after the venous chamber before blood entry into the bloodline of the patient (Jonsson, Drybcak 2022).
In another study foam was detected in the Artis bloodline during dialysis. Follow up studies revealed a problem with the autopriming and advices to the manufacturer who updated the autopriming software. The extent of visible foam was greater with a larger surface area of the dialyzer and for HDF dialyzers(Jonsson 2018).
The Swedish Medical Product agency approved a clinical study using the Emboless® venous chamber and to compare with the Fresenius 5008 bloodline venous chamber. The randomized self-cross over study revealed a significantly better removal of microbubbles at the outlet line of the venous chamber with Emboless ( a median of 76% reduction) versus with the Fresenius 5008 chamber ( a median of 39%, p<0.001).
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept All”, you consent to the use of ALL the cookies. However, you may visit "Cookie Settings" to provide a controlled consent.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-advertisement
1 year
Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Advertisement" category .
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.